
Patients with chronic kidney disease (CKD) often present with a variety of oral manifestations that can significantly impact their oral health and quality of life. CKD is a progressive condition characterized by the gradual loss of kidney function over time, leading to systemic complications affecting various organs and systems, including the oral cavity. Understanding these oral manifestations is crucial for dental professionals in providing comprehensive care for CKD patients.
One of the most common oral manifestations of CKD is xerostomia, or dry mouth, which results from decreased salivary flow. This reduction in saliva production can lead to discomfort, difficulty in speaking and swallowing, increased risk of dental caries, and oral infections. Xerostomia in CKD patients may be attributed to multiple factors, including medications (such as diuretics and antihypertensives), dehydration, electrolyte imbalances, and systemic inflammation.
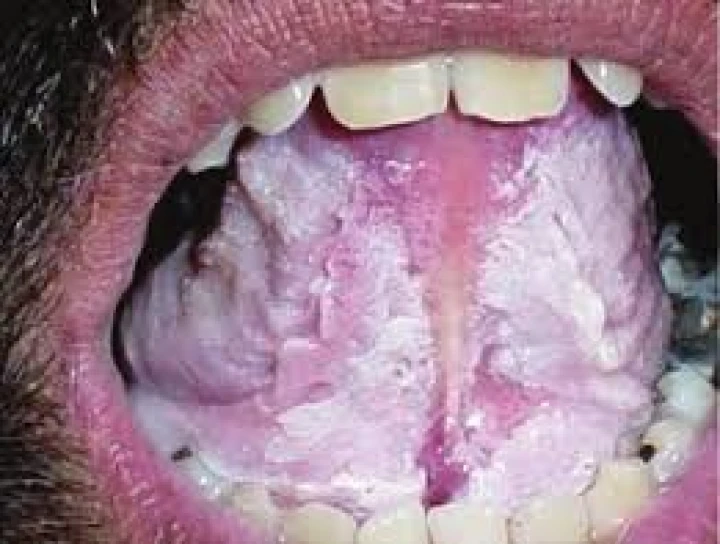
Furthermore, CKD patients are prone to developing oral mucosal lesions, such as uremic stomatitis and uremic frost, as a consequence of elevated blood urea nitrogen levels and metabolic disturbances. Uremic stomatitis is characterized by erythematous or ulcerative lesions on the oral mucosa, often accompanied by halitosis and metallic taste sensations. Uremic frost, a rare manifestation, presents as crystalline deposits of urea on the oral mucosal surfaces, particularly the lips and gums, and is indicative of severe uremia.
Another significant oral manifestation in CKD patients is periodontal disease, which encompasses gingivitis and periodontitis. Periodontal disease is exacerbated in CKD due to immune dysfunction, impaired wound healing, and altered inflammatory responses associated with renal dysfunction. CKD patients may exhibit increased gingival inflammation, gingival bleeding, periodontal pocketing, and tooth mobility. Moreover, periodontal pathogens and inflammatory mediators released during periodontal disease have been implicated in the systemic inflammation and cardiovascular complications observed in CKD patients.
Additionally, CKD patients are at a higher risk of dental caries, enamel defects, and tooth loss compared to the general population. Chronic kidney disease-related mineral and hormonal imbalances, such as alterations in calcium and phosphate metabolism and vitamin D deficiency, contribute to the development of dental hard tissue abnormalities, including dental fluorosis, enamel hypoplasia, and dentin defects. These structural abnormalities compromise the integrity of the tooth enamel, rendering CKD patients more susceptible to dental caries and tooth decay.
Furthermore, oral bleeding tendencies and prolonged bleeding following dental procedures are common in CKD patients due to uremia-induced platelet dysfunction and impaired hemostasis. Therefore, careful management of oral hygiene practices and preventive measures, such as the use of soft-bristled toothbrushes and avoidance of traumatic procedures, are essential to minimize the risk of oral bleeding complications in this population.
In conclusion, chronic kidney disease is associated with a spectrum of oral manifestations that can have significant implications for oral health and overall well-being. Dental professionals play a crucial role in recognizing and managing these oral manifestations through comprehensive assessment, tailored treatment planning, and interdisciplinary collaboration with nephrology and medical teams. By addressing oral health issues in CKD patients, dental professionals contribute to improving the quality of life and reducing the systemic complications associated with this chronic condition.
No Any Replies to “Oral Manifestations of Patients with Chronic Kidney Diseases”
Leave a Reply