
Regenerative endodontic procedures are biologically based procedure designed to restore function to a damaged and non functioning pulp by stimulation of existing stem and progenitor cells present in the root canal and the introduction and stimulation of new stem and dental pulp progenitor cells into root canal under conditions that are favourable to their differentiation and reestablishment of function . Regeneration of tissues rather than replacement with artificial substitutes is an emerging and exciting field in the health sciences. In the near future, it will probably be possible to generate a complete vital tooth from a single stem cell.
Pulp revascularization can be considered as a current alternative treatment to apexification, recommended for immature teeth cases, requiring endodontic treatment. Apexification involves long-term periodic exchanges of a calcium hydroxide paste into the root canal to induce the formation of a calcified barrier. Despite being the most classically therapy employed for these cases, the permanence of calcium hydroxide for long periods of time and also the successive changes may lead to a weakening of the root due to its hygroscopic properties and the proteolytic activities of calcium hydroxide, increasing the risk of fractures and contamination of the pulp space. Thus, a constant search for new treatment alternatives that provide the end of root development have been done to avoid the risk of future root fractures. So, revascularization has emerged as a new treatment option for cases of undeveloped teeth, that provides not only apical closure, as apexification, but also increase the dentin walls thickness.
HOW DOES REVASCULARISATION HAPPENS?
There are a number of theories that explain the revascularization mechanism. The periapical region of immature teeth presents multipotent periodontal cells with great potential for differentiating into new fibroblasts and cementoblasts. So, it has been suggested that differentiated cementoblasts and fibroblasts are responsible for increasing dentinal walls and apical closure. Another hypothesis suggests that residual multipotent stem cells from pulp tissue may be abundant in young, immature teeth, adhering to dentinal walls to generate odontoblast-like cells for root-end development. A third possibility involves the ingrowth of stem cells from apical papilla that could proliferate inside root canals through the blood induction of periapical tissues, since these cells have high proliferative capacity, probably being transported inside root canals in association with bleeding induced from the periapical tissue. In addition to the abovementioned hypothesis, various growth factors incorporated in the blood clot and/ or dentin may play an important role in the cell proliferation inside the root canal space. Finally, the root anatomy of immature teeth (e.g. presenting open apex, wide root canal and thin radicular dentin walls) may favour the communication of canal space and periodontal tissue to achieve apical healing with periodontal tissue.
MATERIAL AND METHODS
Revascularization is a new treatment method for immature necrotic permanent teeth. Indeed, it would provide, after treatment, a vital tooth that would be able to complete its root maturation. Apexification procedures were applied for these teeth:(i)using calcium dihydroxide to induce the formation of an apical calcified barrier;(ii)using mineral trioxide aggregate (MTA) to produce an artificial apical barrier. Both methods have shown to be effective regarding the narrowing of the apical foramen of an immature tooth.
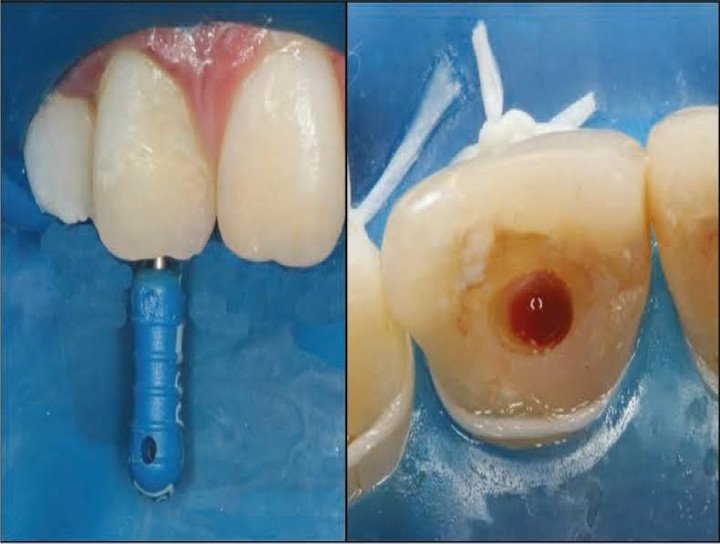
Pulp revascularization is generally performed over two clinical sessions. In the first session, root canals are cleaned through copious irrigation with chemical substances like 3% hydrogen peroxide and 2.5% sodium hypochlorite solution, followed by dressing with calcium dihydroxide as an intracanal medicament for three weeks. After this period, a blood clot is induced and sealed with Mineral Trioxide Aggregate (MTA).
A pilot clinical study was conducted to see the efficacy of revascularisation to induce apexification/ apexogenesis in which fourteen cases of immature, nonvital maxillary anterior teeth presenting with or without signs and/or symptoms of periapical pathology
The results of the study were striking showing complete resolution of clinical signs and symptoms and appreciable healing of periapical lesions in 11 cases. Thickening of lateral dentinal walls could be appreciated in 8 of the 14 cases, and increased root length was observed in 10 of the 14 cases. None of the cases presented with pain, reinfection, or radiographic enlargement of pre-existing apical pathology. Overall, the response to revascularization procedure could be rated as very satisfactory.
CONCLUSION
Pulp revascularization represents a recent and promising therapy for immature teeth, recommended as an alternative to apexification in cases of endodontic treatment of irreversible pulpitis and pulp necrosis, whether or not associated with periapical lesion. It is a technically simple treatment with advantageous outcomes because, unlike apexification, it promotes thickness of the dentin wall width and apical closure, avoiding weakening of the tooth. However, considering that it has only recently begun to be applied, little is known about long-term side effects. Further clinical studies with long-term follow-up may contribute to an understanding of the composition and mechanical properties of the mineralization developed in the inner dentinal walls. In addition, the need for endodontic retreatment and intracanal post rehabilitation in revascularized teeth must be planned in order to extend immature tooth longevity and improve future prognosis.
No Any Replies to “REVASCULARISATION: NEW REGENERATIVE ENDODONTIC PROCEDURE”
Leave a Reply